Patellofemoral syndrome - normal and abnormal patella movement
he healthy, uninjured patella glides, straight up and down vertically in a cartilage-covered groove between the condyles, which are two prominent knuckle-like bones of the femur.
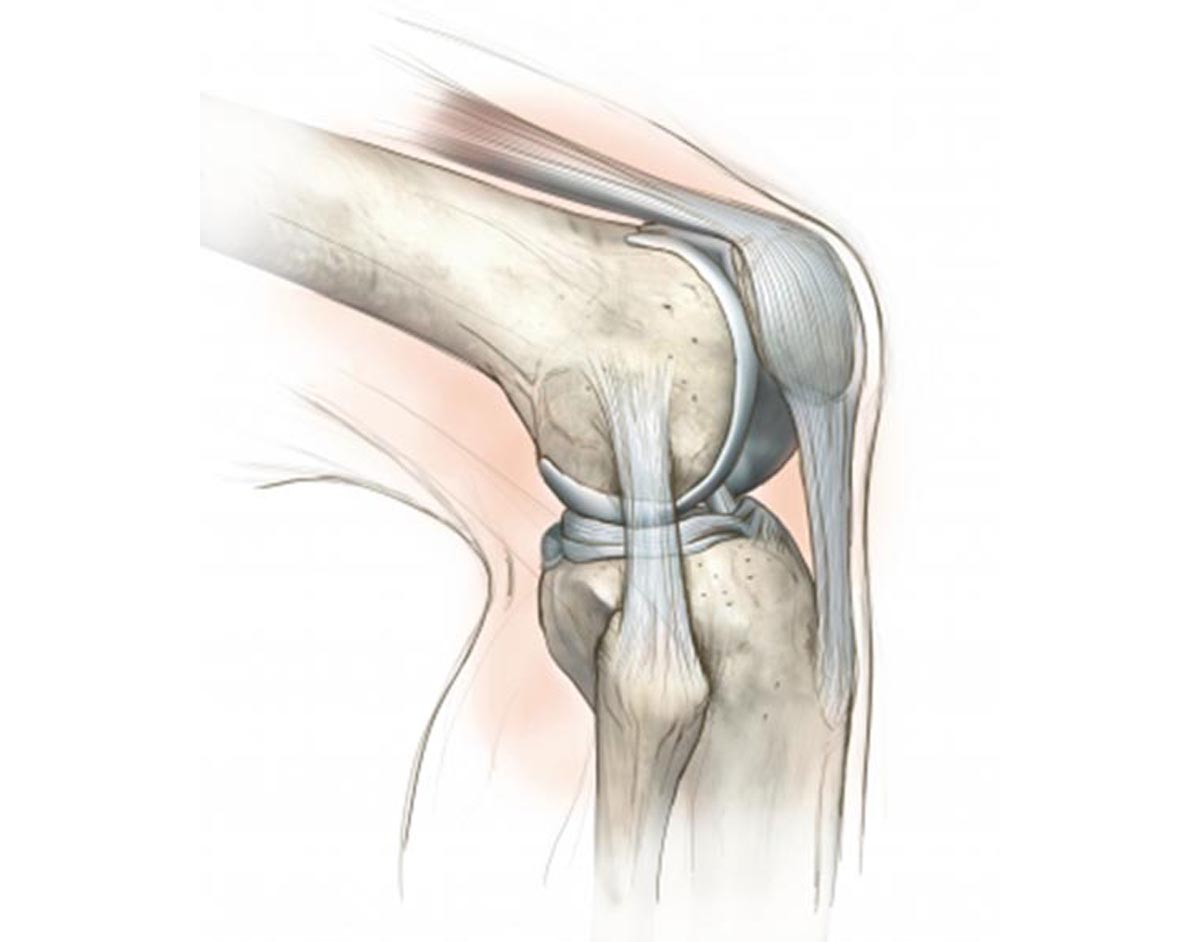
Normal patella movement
During normal knee flexion and extension, the patella lies above and between the condyles, in contact with the suprapatellar fat pad. As the knee flexes, tension in the quadriceps femoris tendon and the patella tendon compress the patella into the femoral condyles, the space between the two protuberances of the femur. The patella is contained within the femoral groove by the height of the medial and lateral femoral condyles, the muscular tone and balance between the muscles adjacent to the patella and the strength of the ligaments attached to the patella.
Abnormal patella movement
When a running injury occurs, and in the event of a patellofemoral syndrome, a tightness of the lateral muscles and ligaments and a weakness of the vastus medialis muscle occurs. This causes the movement of the patella to be disrupted and to deviate laterally from its normal up-and-down path as the quadriceps tendon contracts. Also, a poorly developed femoral condyle can allow the patella to slip further laterally to cause even more of a distorted patella track.
Physical Examination of your knee
A careful examination of the site of injury reveals any anatomic or biomedical malalignments that may have contributed to the cause of the injury. Wearing running shorts only and barefoot, any gross abnormality of the spine, lower limbs, as well as malalignment of the back, pelvic area, legs and feet can be seen. Abnormalities of the knee and patella, such as knock-knee, bowleg, off-center patella, or high-riding patella are indications of problems within. Runners with knee pain often have a malalignment syndrome: a broad pelvis, knock-knee, excessively loose patella, and one or both turned-in feet. X-rays are essential in the evaluation of many knee injuries.
Tip: An inspection for signs of wear on the sole of the running shoe itself can indicate the areas of greater stress. Wear in the front area indicates a forefoot runner, wear on the later sole indicates a turned in foot. Wear on either side of the heel is very common and, if excessive, may be the cause of lateral knee pain.
Symptoms of Patellofemoral syndrome
Patellofemoral syndrome can occur in any runner, but is more common in a runner who is increasing mileage. The pain is described as an ache or soreness around or under the kneecap. It is aggravated by stair climbing or uphill running. The pain may lessen during the run, only to recur when the run is over or at the end of the day. The first episode of pain usually occurs after the run followed by a prolonged period of sitting, or from a fall causing a direct blow to the patella.
Routine questions should be addressed to determine if an overzealous, improper or recently-changed training routine contributed to the cause of the injury. Therefore, knowing the answers to these questions may be able to avoid a lot of wear and tear by isolating and finding the correct problem instead of arriving at wrong solutions:
- When the symptoms were first noticed?
- What kind of activities increase or decrease the degree of discomfort?
- What therapeutic measures have been applied?
- How far and how often do you usually run?
- What type of shoe do you wear?
- Are stretching and warm-up exercises done before running, which ones?
- Has there been sudden changes in routine, course or shoes?
Treatment of Patellofemoral syndrome
Ice and heat. In many cases the use of ice and moist heat is sufficient to allow healing to occur. When a running injury occurs and knee pain is present, the runner should apply ice immediately to the area for 10 to 15 minutes or until the skin turns red. After the first day, the ice treatment is replaced with moist heat for 15 minutes at a time several times a day.
Rest and training changes. Complete rest is necessary for severe symptoms. Otherwise, just a drastic reduction in mileage may be sufficient. If a training error is the cause of the injury— the routine must be revised. A change in the running surface, avoiding hills and banked areas, extended warm-up exercises and new running shoes. Sometimes a totally different non-running program has to be substituted for the runner to help maintain both mental and physical fitness during the healing period. Swimming, cycling, rowing and weight training are all beneficial activities.
Medications and surgery. Oral over-the-counter medications, including Aspirin, acetaminophen, and other NSAID’s (non-steroidal anti-inflammatory drugs) such as ibuprofen and naproxen should first be tried to help reduce the swelling and alleviate the pain. For more severe pain that is persistent, opioid agonists (combatants) such as morphine and codeine derivatives may be administered with a doctor’s prescription. Corticosteroid injections are infrequently needed but may be advised if complications arise such as bursitis, tendonitis or torn ligaments or muscles in the knee area. Surgery is even less frequently performed.
Prevention of Patellofemoral syndrome
When pain-free and asymptomatic, the runner can begin a graduated training/prevention program using the following guidelines:
- Before training, apply moist heat to the knee area for 5 minutes
- Warm-up with low-impact calisthenics, walking 3 to 5 minutes
- Stretching exercises
- Alternate walking and running
- Ice massage to the knee area for 10 minutes (even with no pain present)
- Apply moist heat at night for 20 minutes
Alternate walking with running for the first 2 weeks after returning to your routine. On alternate days, substitute other types of exercise. As long as there are no symptoms present, gradually reduce the walking portion and increase the distance run slightly until the original level of training is reached. This may take 4 to 6 weeks. Whatever course of action you take to rehabilitate, do not ever “work though” or “run out” your injury— the body just doesn’t heal that way.
Several exercises to relieve knee pain:
- Cox, J.S. Patellofemoral Problems in Runners, Clinical Sports Medicine, 1992
- Lutter, L.D., M.D., The Knee and Running Clinical Symposia, Vol.32, 1995
- Aronoff, GM, M.D. Handbook on Rational Use of Medication for Pain, 1997