Table of Contents
We all heard about cholesterol. Most people are well aware of connection between high level of cholesterol and heart problems. Cardiovascular diseases are the single largest cause of mortality in Western world, and most of these diseases are closely connected with the dis-balance of cholesterol in the body.
Cholesterol is not necessarily bad. After all, this is one of the major components of our cell membranes. Our body simply won’t be able to function without cholesterol. Every day our body produces, on average, 1g of cholesterol to cover its needs in this biochemical compound. Problems come with the excess level of this essential biochemical in the blood.
Essentials of cholesterol metabolism
Cholesterol in our body originates from two major sources. It is produced by various organs and tissues in our body (for example, liver), and it also comes from our food. In people with healthy diet, food contributes to around 20% of all cholesterol. Obviously, unhealthy diet has a potential of increasing the cholesterol intake rather significantly. But what actually happens when the blood cholesterol rises to the dangerous levels?
Cholesterol is needed by each and every cell in the body. This means that it has to be delivered to all these cells from where it is produced or ingested. Also, the excess of cholesterol should be properly removed (this task is fulfilled by the liver as well) and disposed of. Cholesterol molecules must be able to travel around the body.
There is one problem here, however. Cholesterol is not soluble in water. If you take chemically pure solid cholesterol and try to mix it in a glass of water, it will simply precipitate to the bottom of the glass. Insolubility of cholesterol means that it is also not soluble in blood. And this creates problems with its transportation around the body.
Our body solved the problem by providing cholesterol with special carrier proteins in the blood plasma. These proteins are capable of binding cholesterol molecules on their surface and transporting them in the blood around the body. The binding is reversible, and cholesterol molecules can be released when they reach their destination.
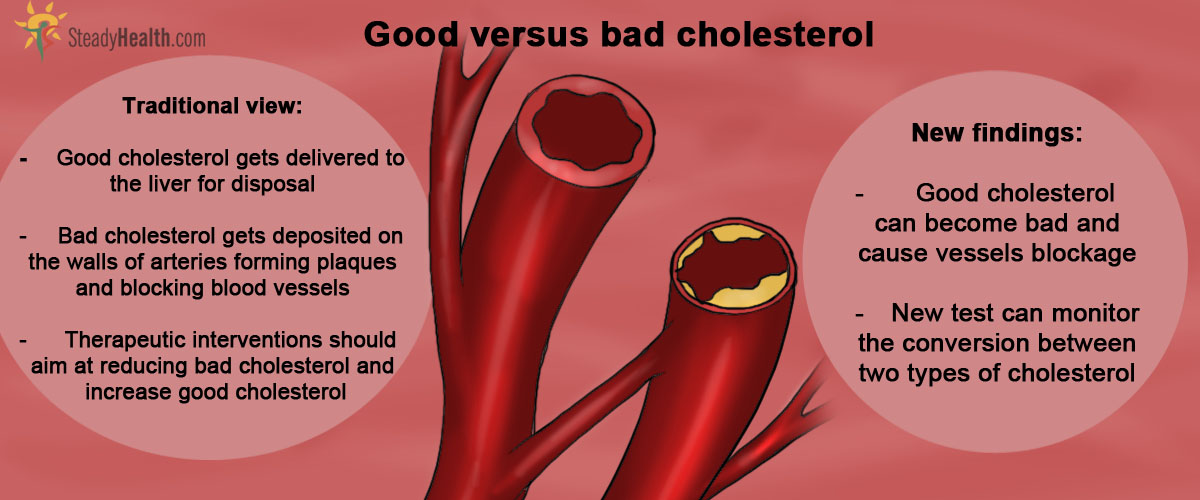
“Good” cholesterol and “bad” cholesterol
Many of us heard of so-called good and bad cholesterol. Well, the names are slightly confusing. There is no chemical difference between these two types of cholesterol, both are exactly the same compound. The difference is in the type of carrier protein to which cholesterol is bound. Our blood contains two major type of cholesterol transporter – High Density Lipoproteins (HDL) and Low Density Lipoproteins (LDL).
See Also: The Myth Of The Cholesterol Myth
Why? Because HDL binds cholesterol quite tightly which enables it to be successfully delivered to its destination, while LDLs are not very good at keeping cholesterol molecules and tend to lose them during transportation. Once free cholesterol is released from LDL, it becomes insoluble and precipitates on the walls of blood vessels.
For some reason, the precipitation of cholesterol is particularly active on the walls of blood vessels supplying our heart. It can also be deposited on the walls of aorta and in the blood vessels of the brain. Deposits of cholesterol are known as cholesterol plaques. Over time, these plaques grow and start to block the affected blood vessels. This eventually leads to the lack of blood supply to various tissues and organs, which start to suffer from the lack of oxygen and nutrients. Ischemic heart disease, aortic aneurism, stroke and myocardial infarction are all caused by formation of cholesterol plaques. LDL-bound “bad” cholesterol is considered the major villain in their development.
- Rhodes CM Stryer L, Tasker R (1995). Biochemistry (4th ed.) San Francisco: W.H. Freeman. pp. 280, 703
- Ascherio A, Willett WC (October 1997) Health effects of trans fatty acids. Am. J. Clin. Nutr. 66 (4 Suppl): 1006S–1010S
- Castelli WP (July 1992) Concerning the possibility of a nut... Arch. Intern. Med. 152 (7): 1371–2
- Demonty I, Ras RT, van der Knaap HC, Duchateau GS, Meijer L, Zock PL, Geleijnse JM, Trautwein EA (February 2009) Continuous dose-response relationship of the LDL-cholesterol-lowering effect of phytosterol intake. J. Nutr. 139 (2): 271–84
- Ying Huang, Joseph A DiDonato, Bruce S Levison et al. (26 January 2014) An abundant dysfunctional apolipoprotein A1 in human atheroma. Nature Medicine. Early online publication.
- Mindmap by steadyhealth.com
- Photo courtesy of ThisParticularGreg by Flickr : www.flickr.com/photos/thisparticulargreg/514871141/