What are Uterine Fibroids?
Uterine fibroids are fibroid tumors that develop in the uterus. The fibroid part simply means that the tumor contains or resembles fibers. They consist of a fibrous capsule that contains the blood vessels that supply the tumor with blood. Fibroids are benign, non-cancerous.

Fibroids usually develop in multiple locations concurrently and their location is the descriptor used in diagnosis. There are four types: myometrial, submucosal, subserosal, and pendunculated. Myometrial fibroids develop in the uterine muscle wall. Submucosal fibroids are found under the surface of the uterine lining. Subserosal fibroids refer to those located just under the outside surface of the uterus. Pendunculated fibroids are those that grow at the end of a stalk, like the bud of a flower. These can grow in the uterine cavity or outside the uterus.
How Do I Know if I Have Uterine Fibroids?
Most likely, you won't know until you're at least 30 or so. It's rare for fibroids to cause any symptoms before then. The fibroids themselves don't start growing until age 20 in most cases and they have to get to a pretty good size before they begin to affect the uterus.
The typical symptoms that reveal their presence are dysmenorrhea (painful menstruation), menorrhagia (heavy and/or prolonged menstruation), and leukorrhea (white vaginal discharge). However, all of those symptoms depend on where the fibroids are in the uterus. Fibroids at the top of the uterus may increase pressure on the bladder and result in frequent urination instead of the more typical symptoms. Those near the bottom may produce a persistent sensation of needing to have a bowel movement. Subserosal fibroids may not produce any symptoms at all, even at very large sizes.
What's the Big Deal Then?
Well, the biggest issue is that some fibroids are big enough and in the right location to affect a woman's fertility. A large mass that takes up most of the space in your uterus isn't exactly conducive to a healthy pregnancy and can lead to premature birth. Fibroids can also get larger during pregnancy because of higher levels of blood flow to the uterus, as well as increased estrogen levels. In some cases, they can even block the birth canal, necessitating a caesarean section at delivery.
Fibroids can also have some nasty complications. Severe pain and heavy bleeding can actually lead to emergency surgeries. Very heavy bleeding can cause anemia.
Read More: Endometrial/Uterine Cancer
Some fibroids can twist around also. With blood vessels linked to the tumor, the twisting can cause a blockage that requires surgery to correct. In very rare cases, cancerous changes can occur in fibroids.
Still, many women with fibroids remain asymptomatic and never require treatment, other than monitoring of the tumors for suspicious signs, such as rapid growth. So, how does one monitor a uterine fibroid?
Diagnosis And Treatment Of Uterine Fibroids
Diagnosing Uterine Fibroids
The first step in diagnosing uterine fibroids is a simple pelvic exam. Your doctor will palpate (examine by touch) your uterus to feel for any abnormalities. Unfortunately, this isn't always an accurate diagnostic. The fibroids may be positioned in a way that makes them undetectable by simple touch.
The next step taken is an ultrasound. This can be a transabdominal ultrasound with the doctor moving the transducer over the abdomen, or it can be done transvaginally with a transducer inserted into the vagina. Either way, the ultrasound allows the doctor to visualize the uterus and determine the presence of uterine fibroids.
In some cases, such as when abnormal bleeding is present, your doctor may request a pelvic MRI. An MRI provides a clearer picture of the uterine anatomy than an ultrasound. It allows better measurements to be taken of any fibroids that are present. It also helps your doctor to see if any of the fibroids are degenerating or deteriorating.
Finally, if your doctor suspects that any uterine fibroid is cancerous, he or she will order a biopsy.
Treatment Options
For uterine fibroids that are asymptomatic, no action is necessary. Non-surgical techniques for managing symptomatic uterine fibroids include oral contraception and IUDs to reduce heavy bleeding, iron supplements to treat anemia caused by heavy bleeding, and over the counter medications such as ibuprofen for pain. All of these options only treat the symptoms, though, and they all come with their own risks and side effects. There is the option of short-term hormone therapy to shrink the fibroids. Luteinizing hormone-releasing hormone (LHRH) can be injected, but the tumors will return when the therapy ceases.
To really get rid of fibroids, surgery is necessary. There are a few methods that are utilized. Hysteroscopy (inserting an endoscope into the uterus) allows a surgeon to remove fibroids by electrocautery. The fibroids are cut away and the blood vessels are cauterized at the same time with an electrically-charged tool.
Read More: Intrauterine Devices: A Contraceptive Option More Women Should Consider
Another method is uterine artery embolization. During this outpatient procedure, the patient is lightly sedated while a catheter is inserted into the femoral artery and threaded up to the uterine artery. Special particles are released into the blood vessels that supply the fibroids, blocking them and choking off the fibroids' blood supply. While the procedure itself is low-risk, it may affect fertility and cause problems with future pregnancies. Therefore, this procedure is generally recommended for women whose families are complete. For women who want to have children in the future, a myomectomy is preferred. This is a direct removal of the tumor and usually does not affect fertility.
The last resort for treatment is a hysterectomy, which is the complete removal of the uterus. This is a highly-invasive surgery and is only used when no other options are available. Obviously, a hysterectomy renders a woman infertile. For those of child-bearing age, it would be a serious decision to be made between patient and doctor.
- Uterine fibroma. (2001). In Taber's Cyclopedic Medical Dictionary (pp.761-762, Edition 19). Philadelphia, PA: F. A. Davis Company.
- Photo courtesy of Quinn Dombrowski by Flickr : www.flickr.com/photos/quinnanya/3706412802/
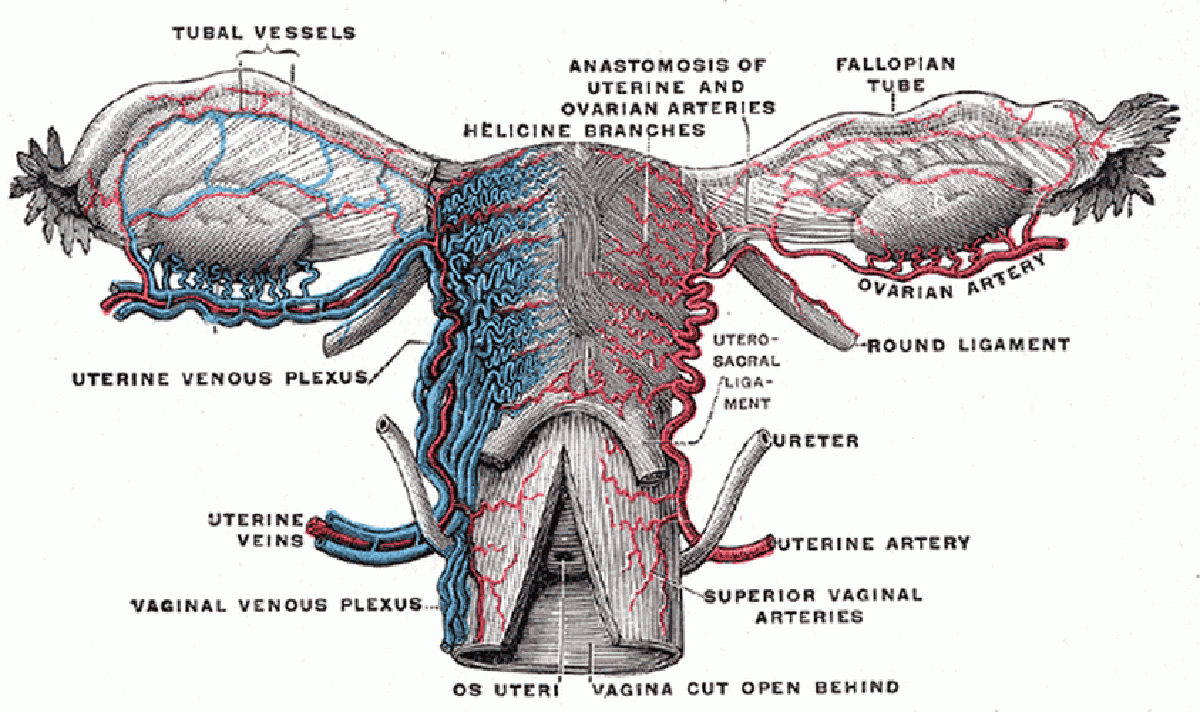
- Photo courtesy of Arcadian by Wikimedia Commons : en.wikipedia.org/wiki/File:Gray589.png